Pelvic Health & Orthopedic Physical Therapy
Addressing your questions about pelvic, women's, and musculoskeletal health. Health is a journey. Movement is healing!
|
You went to the bathroom an hour ago, now you have to go again. In twenty minutes you will have to go to the bathroom once again. You will desperately need to find a restroom. Your life revolves around frequenting the bathroom to urinate, but when you go it doesn't always seem like all that much urine.
Does this sound like you? You may be experiencing the symptoms of overactive bladder. Individuals with this typically urinate more than eight times a day. When they do need to use the restroom, they are overcome with an intense urge to urinate. The urge make even lead to some urine leakage at times. When you do get to the restroom you quickly empty your bladder and head about your business, just to quickly rush back to the bathroom shortly. Why does this happen? Sometimes there is an underlying medical reason, other times we develop poor bladder health and train our bladder to go more often.So what can you do? A good first step if you suspect you have overactive bladder is to visit your physician. They can start medical management such as medications if necessary. You may also get referred to Physical Therapy to work on your pelvic floor muscles and retraining the bladder and your current bladder habits. Have you heard of painful bladder syndrome sometimes it's referred to as interstitial cystitis (IC)? It can be really tricky to diagnose so it could be years before getting diagnosed properly and receiving the right treatment. Some individuals just think they are continuing to get UTI’s even though the tests are negative. What is IC exactly? Even the definition is a bit tricky. The thought is interstitial cystitis is result of the lining of the bladder not functioning properly so the acidic contents of the bladder irritate the bladder wall. The body goes into an overdrive mode stimulating an inflammatory response and increasing the chemicals that make your body experience pain. The reason this occurs is not fully understood. Some studies point to genetic reasons, others say its root is in multiple bladder infections like UTI’s. When the organs have this reactions they have an effect on the musculature of the pelvic floor coupled with the pain that is experienced which leads to overactivity and tight musculature. When the body develops this response it can either happen over a long amount of time or quickly. It is a painful syndrome, but can fluctuate in nature. So you will go through times of feeling okay and then times of intense pain. Pain is usually worse when you have a full bladder and is in the pelvic region primarily, but can occur elsewhere. You also may experience the need to get up during the middle of the night to use the bathroom. You might feel like you have to use the restroom more often or when you have to go you REALLY have to go! Pain may get worse around the time of your period. You may have pain with intercourse and following intercourse for a few days. If you feel like you are experiencing these symptoms and haven’t been treated the best place to start would to seek an appointment with a urologist or urogynecologist. They will run some tests to verify what is going on, help to get you on the correct medications, and possibly refer you to Pelvic Physical Therapy. There are a lot great websites out there with information. Here are just a few to start finding more resources. https://www.ic-network.com/ https://www.ichelp.org/ http://www.ic-today.com/ https://pelvicpain.org/home.aspx  Do you ever laugh so hard a little pee just leaks out? Or maybe you are a cross-fit athlete and every time you do a lift you just leak a few drops. You just had a baby a few years ago and you never felt quite the same and now you notice when you gotta go to the bathroom you better start running or you end up with a little urine running down your leg. Maybe you constantly wear a pad or carry around extra panties due to fear of an accident. Try as you might, you lose a little bit of pee, maybe it's even more than a small amount. This is called "urinary incontinence" when you unintentionally lose urine and there are a few different types. Stress Incontinence is when you accidentally lose pee. It can be with certain activities like coughing, sneezing, laughing, running, or when you stand up for sitting in a chair. These types of activities can change the pressure in your abdomen which influences your bladder and pelvic floor. If the muscles of your pelvic floor are weak they may have a difficult time staying closed to stop urine from coming down that urethra we talked about in the previous post. Urge Incontinence is when you accidentally lose urine with a strong urge to use the restroom. So you feel like you have to go to the bathroom and with the urge you lose control of your bladder and have a leak. The bladder has trained itself that it's time to go so you cannot wait. Oftentimes this is a mixture of pelvic floor musculature being both tight and weak. Functional Incontinence is when you physically cannot make it to the restroom so you have leakage. This could be that you are bed bound, unable transfer to the toilet on your own, or unable to unbutton your pants due to issues with dexterity in time causing loss in urine. So when does incontinence occur? Different types of incontinence can occur throughout different stages of life or with different conditions. Women commonly develop incontinence after giving birth and/ or after menopause. This can be due to the pelvic floor musculature going through changes as well as changes in hormones. And despite being told that this is "just old woman bladder" there is definitely techniques Physical Therapists can help you implement to better control your bladder. For men urinary incontinence and urgency can develop in individuals who have their prostate removed.  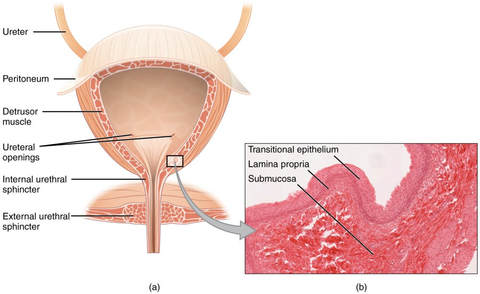 Overall the bladder is pretty impressive. November is a time to recognize the bladder and different ways the bladder can be affected. We don't really think about how the bladder functions until something isn't functioning the way we want it to. So this month I am going to blurbs about the bladder and conditions that can change how the bladder functions. Let's begin with a crash course on the anatomy of how the bladder functions. The kidneys are connected to the bladder by ureters. The kidneys are responsible for filtering particles out of the urine before it passes to the bladder. The bladder functions as a storage unit for the fluid waste exiting your body. The bladder is hollow, it gets bigger as you drink. The bladder has a protective inner layer to protect it from the fluid inside. The muscles around the bladder and nervous system work together to store and release urine. The detrusor muscle surrounding the bladder relaxes to store urine and contracts to release urine. The detrusor muscle works with the urethral sphincters and pelvic floor musculature to properly release urine. The sphincters are circular openings surrounded by muscles, the muscles contract to close and relax to open. The bladder connects and empties into the urethra, the tube-like structure which allows for urine to leave your body. Now for men things are a little bit different as they have some extra anatomy around the urethra, the prostate. 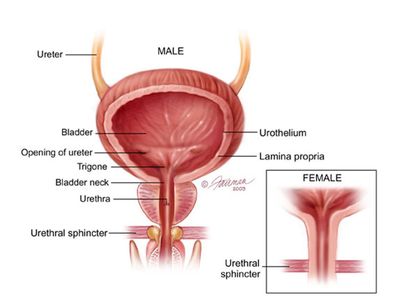 When the bladder becomes full it sends a message to the brain that it is full and needs to use the restroom. When the bladder sends the signal we make the conscious decision whether we want to use the restroom or put it off for a bit longer. So we have voluntary control over the bladder.
There you go! Now you have a summary on how the bladder functions! References: Image 1: https://courses.lumenlearning.com/ap2/chapter/gross-anatomy-of-urine-transport/ Image 2: http://slideplayer.com/slide/3408814/  Here in the United States we sit on toilets where are legs are at 90 degrees or even larger angles. Guess what? That is not the ideal position for having a bowel movement in fact, if you are already straining being in this position will only make having a bowel movement more difficult. We have a muscle in our pelvis, the puborectalis, that runs from the front of the pelvis back around the rectum and then connects back to the front of the pelvis again. It forms a sling basically. When we sit at a 90 degree angle this muscle cannot fully relax allowing the contents of the rectum to pass through as picture below on the left side. It's as if you take a garden hose and kink it slightly, the contents won't pass through as readily. The solution is to get into a squatting position. How do you do this? Have you heard of a Squatty Potty? If you haven't you need to add it to your Amazon wish list ASAP. In the picture on the right you can see how the position of the puborectalis and the colon changes with the squatting position (hips are both bent and the back is bent forward slightly--not hunched). The colon can more easily empty in this position without you feeling like you need to strain to empty your bowel. You can also use a stool to elevate your feet on the toilet to assume the squatting position, but I think the Squatty Potty is pretty nifty because it's the perfect height, comes in different sizes, plus it slides right under the toilet when you are done. Some other tips to avoid straining: 1. Try to relax when on the toilet. It does no good to sit there just pushing continuously. 2. Keep your mouth open when you are breathing so that you don't increase the pressure in your abdomen. 3. Give yourself enough time, about 10 mins. If you don't go in 10 minutes get up and walk around, try again at a later time. This may not apply to all individuals if you are concerned about your ability to have a pain-free bowel movement please see your local pelvic health physical therapist. 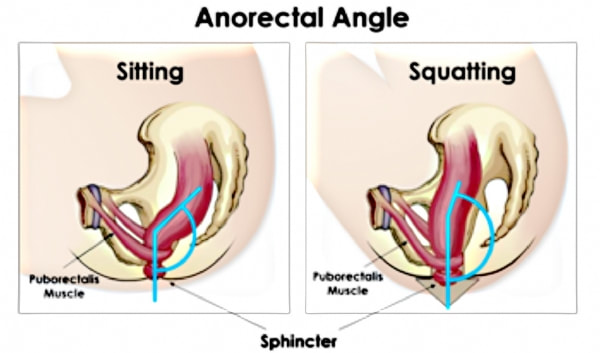 It's October again. I know the hospital I work at is all decked out in pink. Awareness regarding breast cancer is everywhere. It's in the grocery store, there are races, it's even worked into the media. Awareness about the risk of developing breast cancer and celebration of survivorship are pretty apparent. Some of the struggles of survivorship are not as readily discussed. One issue that some women can face after treatment for breast cancer is perineal discomfort, urinary incontinence, and even pain with intercourse. One of the biggest challenges for those navigating survivorship is things can be very overwhelming. There are a lot of financial, emotional, physical, and physiological impacts of fighting and surviving breast cancer that these individuals must face. It is sometimes difficult to find where physical intimacy and pelvic issues fit into the picture. Treatment for this type of cancer targets hormones in the body which can impact the tissues in the pelvic region. As a result discomfort, loss of urine, or pain with physical intimacy may occur. The muscles of the pelvic floor need estrogen and progesterone to function so by quickly removing them, the muscles don't know how to properly react. The muscles of pelvic floor may begin to develop weaknesses or areas of tenderness. The tissue integrity may change as a result of previous treatment. So when you are ready to seek treatment pelvic health physical therapy can help to address the changes that these tissues have experienced. With this type of PT they will look to restore improved tissue quality and provide the individual techniques for improved control over those muscles. They can provide insight on different lubricants and ways to decrease irritation from dryness. The PT can help to improve strength, muscle control, and decrease point tenderness. They can also help to trouble shoot different biomechanical difficulties occurring and help develop a plan to decrease accidental loss of urine.  Everybody poops and according to Harris et al 2006 approximately 20% of individuals in the United States suffer from constipation. That's 1 in 5 people you meet have trouble pooping. So I've decided to do a series about constipation! Wohoo! So let's dive right in. It's not really surprising that so many people suffer from issues with constipation. I mean let's just think about some of the things that can contribute to constipation. DIET. We eat a lot of sugar, carbohydrates, and processed foods in America. You know how it feels a little like glue when you are chewing it? That's how it is in your gut as well. Pairing hand in hand with what we eat is what we drink. We don't get nearly enough water throughout the day. If we are lucky we stop to sip on water occasionally or some people avoid water altogether for more caffeinated and sugar-filled alternatives. But our gut needs water. The colon pulls all of the water out whatever is in it, so pair that with your gluey mess from above and you have something that just isn't going to budge very easily when you are sitting there on the toilet. Beyond diet there are some other factors that can contribute to constipation. Certainly the anatomy and motility of the intestines can play a role, but not every person walking around has had some change in the ability of their organs to move food through the digestive system (which is the definition of motility). So what else is there? Your pelvic floor muscles play a large role in the development and continuation of constipation. The muscles can become tight and can have a difficult time relaxing in order to have a bowel movement. Which is where a pelvic health or women's health physical therapist can come in to help alleviate your symptoms. The physical therapist can help to release those muscles, give you relaxation techniques, and then ultimately work on proper positioning and toileting techniques to help alleviate your symptoms of constipation. Symptoms of constipation can influence your overall health and well-being. They can cause you anything from mild to severe discomfort in your low back, abdominal, and perineal areas. I mean it just doesn't feel good when you can't have a bowel movement and you are all backed up. There are changes to diet and techniques physical therapists can help you to implement to offer relief from these symptoms. Stay tuned for part 2 on constipation we'll plunge a little deeper (pun definitely intended).  References:
Harris LA, Hansel S, DiBaise J, Crowell MD. Irritable bowel syndrome and chronic constipation: Emerging drugs, devices, and surgical treatments. Curr Gastroenterol Rep. 2006;8:282–90. Sorry for the hiatus from blogging! I've been settling into my new place and job, things have just been a little bit on the crazy side. Anyways, lots has been going on. So what's new? I recently went to another continuing education course on pelvic health physical therapy. We dove deeper into more complicated topics on gastrointestinal pathologies and pelvic pain. Remember all of those important muscles of the pelvic floor? They can impact your ability to have normal bowel movements. They have to lengthen for pleasurable intercourse. They also play an important role in a variety of pain diagnoses felt in the perineum, back, and legs. Chronic Pelvic Pain is described as pain in your pelvic region lasting longer for 6 months. The Mayo Clinic tweeted just this past week that 39% of women will experience Chronic Pelvic Pain at some point during their lifetime. This is just the number of women currently reporting their symptoms, so the number of women actually experiencing pelvic pain could be much larger. Many women just don't know who exactly to turn to for help. I just want to say that there are a lot of ways to help manage that pain and Pelvic Floor or Women's Health Physical Therapists can help patients with not only this type of pelvic pain, but many diagnoses. You see when our body experiences pain A) the muscles form a muscle memory and B) the muscles tighten and guard against the pain. If that pain stimulus does not subside our body continues to become more sensitive to pain triggers so smaller triggers elicit a greater pain response. This is true for ANY aspect of our body, including the muscles of the pelvic floor. So what does mean for an individual experiencing pelvic pain? A Pelvic Floor or Women's Health Physical Therapist can help you lengthen and relax your pelvic floor musculature, give you techniques to encourage more positive connections between the brain and muscles, and help to desensitize the area.  I have been a student the last 20 out of the 25 years of my life. It's safe to say I really don't remember a time when I wasn't studying or completing an assignment, on break, or gearing up for the next degree. Don't get me wrong, I love school. At one point in college one of my many career options was to pursue education to become a teacher. I enjoy learning about lots of different things (not so much math and organic chemistry), but school was also a constant source of anxiety in my life because I am very much a "Type A" person. Ever since graduating in May I have still been in school mode because I have been locked away studying for my licensing exam in Physical Therapy. Last week I found out I passed my exam which was such joyful and relieving news, but now I find myself in a space that I haven't been in before. What do I do now that I am done with school? For the very near future I do know what will fill my time. Preparations for my move for my new career! For those of you who do not know I am moving to Carmel, IN (a suburb of Indianapolis) to work for Indiana University Health as a pelvic health Physical Therapist. I'll be a Hoosier once again. It's really my dream job. The patient caseload is really diverse with women, men, and pediatrics as well as a variety of pathologies that I really want to treat! So I am over the moon to pack my bags and head to Indy for this adventure! 
You are 30 years old and one day your back just starts to ache. You went to your doctor, you were prescribed some muscle relaxants, but they really haven't done much to help ease your pain. In fact your pain continues to build. You have stopped doing the things you enjoy, running, hiking, and playing with your kids because you are worried it will make your back hurt more. They only thing that seems to help is lying down. You get an MRI of your back and get the worse news, you have a "bulging disc". Your "back looks 10 years older" than your age. You are sent to Physical Therapy for your "bad" back.
How would you feel if you are the individual in the story? Scared? Leary to move? Worried to return to the activities that you enjoy? Perhaps anxious about the current and future status of your back? Words create a story and are impactful. I remember learning early on in middle school and high school about bias, specifically bias created by language. It is not always evident how words create bias, but the choice in words can change the way a person thinks or behaves. The same is true in the health field. Even in health care the type of language that practitioners use can alter how people think and behave about their diagnoses. Choice of language is paramount in discussing pain and reasons people believe contribute to their pain. As Physical Therapists it is important to listen and empathize when someone is disclosing about pain they are experiencing because pain experiences are very real and personal. However, it is also important to be cognizant of the language PTs utilize with patients as to not perpetuate biases about pain and to properly educate patients about their body and rehabilitate them in order to instill confidence to return to the activities that give their life purpose and joy. In the instance above the individual's Physical Therapist would know that there have been studies showing that some individuals with bulging discs do not exhibit any symptoms of back pain and that a thorough musculoskeletal exam should be completed to determine the source of the pain. These studies includes a literature review performed by Brinjikji et al 2014 where in the studies 40% of the individuals who where 30 years old had imaging done demonstrated a bulging disc without any symptoms of pain. So while diagnostic imaging can certainly be helpful when appropriate at times it may reveal more about a patient's body than may be necessary. For instance, as a healthy 25 year old female if someone took images of my back they may see a bulging disc, but I am not experiencing any symptoms of back pain. Thus a bulging disc is not always primarily causative. The PT would then need to start addressing the patient's possible fear of movement and avoidance. It would also be crucial to start building the individual's confidence in their ability to move and start dispelling the belief that they have a "bad" back. Peter O'Sullivan does a lot of research and education on pain science. He spoke to Dr. Karen Litzy on her Healthy, Wealthy, & Smart podcasts a few months ago about re-examining the way Physical Therapists address pain processes with patients. I highly recommended listening to the full interview! Which you can access here:
http://podcast.healthywealthysmart.com/2017/03/262-prof-peter-osullivan-reconceptualizing-pain/

References:
Brinjikji, W., P. H. Luetmer, B. Comstock, B. W. Bresnahan, L. E. Chen, R. A. Deyo, S. Halabi, J. A. Turner, A. L. Avins, K. James, J. T. Wald, D. F. Kallmes, and J. G. Jarvik. "Systematic literature review of imaging features of spinal degeneration in asymptomatic populations." AJNR. American journal of neuroradiology. U.S. National Library of Medicine, Apr. 2015. |
AuthorHello! I am Caitlyn, Doctor of Physical Therapy and Board Certified Women's Health Physical Therapist working in St Louis, Missouri. Faculty in developing residency program. Endowarrior Categories
All
Archives
July 2021
|
 RSS Feed
RSS Feed
